1. Introduction
The relationship between technology and healthcare has never been straightforward. Innovation tends to arrive with considerable promise, and AI is no different — except perhaps in the scale of what it is being asked to accomplish. Over the past decade, AI-driven tools have moved from experimental settings into clinical and public health practice in ways that would have seemed ambitious only a few years ago. Machine learning models now assist with diagnostic imaging, natural language processing supports clinical documentation, and predictive algorithms help epidemiologists anticipate disease spread before outbreaks fully materialize (Olawade et al., 2024). Whether these developments translate into equitable, measurable improvements in population health is a question the field is still working through.
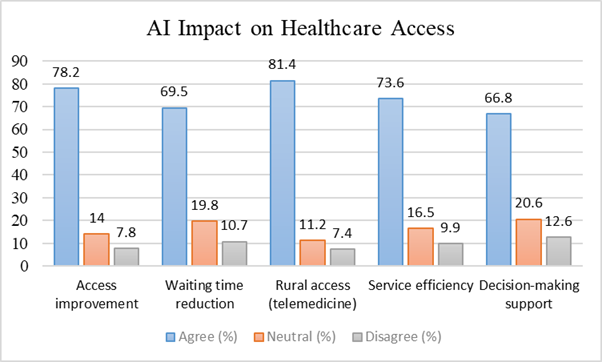
Part of what makes this moment consequential is context. Healthcare systems globally are under strain — patient volumes are rising, chronic disease burden is accelerating, and the workforce required to meet demand is not keeping pace (Rehman et al., 2021). In resource-constrained settings, including many parts of South and Southeast Asia, these pressures are more acute. Rural populations frequently lack reliable access to specialist care, diagnostic infrastructure is inconsistent, and administrative inefficiencies compound the problem (Varnosfaderani & Forouzanfar, 2024). Against this backdrop, AI-based tools — telemedicine platforms, remote monitoring devices, intelligent triage systems — are being positioned not as luxury additions but as potential equalizers (Alowais et al., 2023).
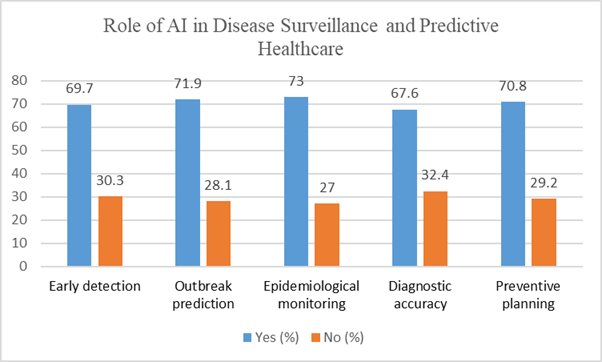
The evidence behind this optimism is, at least in certain areas, reasonably compelling. Studies in radiology and pathology have reported diagnostic accuracy improvements in the range of 20–30% when AI-assisted tools are used alongside clinicians, primarily because these systems can process imaging data at a scale and speed that human review cannot match (Da Silva, 2024). Machine learning algorithms applied to population-level datasets have demonstrated the capacity to identify patterns preceding disease outbreaks, giving public health authorities a degree of early warning that traditional surveillance methods struggle to provide (Prosperi et al., 2018). During recent health emergencies, AI-based epidemiological platforms supported faster, more granular decision-making than many conventional systems could offer (Syrowatka et al., 2021).
Beyond clinical decision support, AI is generating interest for its potential to reduce the operational friction that consumes a disproportionate share of healthcare resources. Administrative tasks — scheduling, documentation, billing — account for a significant portion of clinician time in many health systems (Johnson et al., 2020). Automating or augmenting these processes could, in principle, redirect professional capacity toward direct patient care. AI-driven resource allocation tools have also shown promise in improving bed management, staffing, and equipment utilization, particularly in hospital settings operating near or above capacity (Khalifa et al., 2024; Bekbolatova et al., 2024).
That said, it would be misleading to present this picture without its complications. The same systems that offer efficiency gains also introduce risks that are not trivial. Algorithmic bias — the tendency of models trained on non-representative data to perform unequally across demographic groups — remains a persistent concern in health AI (Mhasawade et al., 2021). Data privacy is another unresolved tension: the value of AI depends on access to large, detailed health datasets, yet the collection and use of such data raise legitimate questions about consent, security, and governance (Williamson & Prybutok, 2024). Implementation costs are prohibitive for many health systems, and the human infrastructure needed to support these technologies — trained staff, interoperable systems, regulatory frameworks — is often absent precisely where the need is greatest (Mandal & Ghosh, 2023).
Much of the existing research on AI in healthcare focuses on technical performance — sensitivity, specificity, model accuracy. Fewer studies examine how the professionals who would actually use these tools perceive their potential, or what barriers they anticipate in practice. This matters, because adoption ultimately depends on institutional willingness and workforce readiness, not just technical capability (Morgenstern et al., 2021). Understanding how healthcare practitioners, administrators, researchers, and technology specialists view AI's role in public health — what they find credible, what they remain skeptical about, and what they see as the most pressing obstacles — offers a ground-level view that technical benchmarks alone cannot provide.
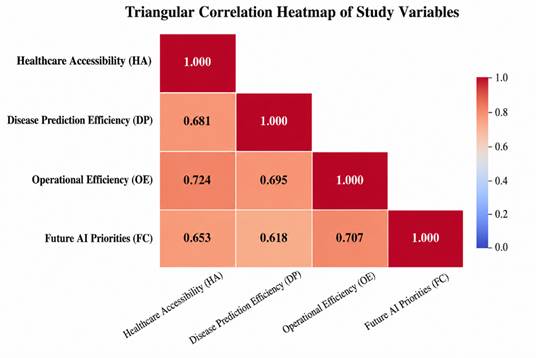
This study was designed to gather precisely that kind of evidence. Through a structured cross-sectional survey of 185 professionals working across health and technology sectors, we examined perceptions of AI across four domains: healthcare accessibility, disease prediction, operational efficiency, and future implementation priorities. The goal was not to adjudicate AI's potential in the abstract, but to understand how those closest to its deployment are thinking about it — and where the real work of integration still lies ahead.