1. Introduction
Skin cancer is, by most counts, one of the most common cancers being diagnosed today (Ashraf et al., 2020) — and that alone would be reason enough to take it seriously. But there's a second, more hopeful fact sitting right next to that first one: when it's caught early, the outlook changes dramatically. Development is often predictable in its early stages (Siegel et al., 2018), which matters enormously for how well and how long a patient goes on to live. Some numbers make this concrete rather than abstract. Patients treated in the early stages of skin cancer see five-year survival rates above 99% (Esteva et al., 2017) — a figure that's almost startling given how differently the story can end otherwise.
Melanoma is where the stakes rise fastest. Left undiagnosed, it doesn't stay put; it moves outward from the original site into surrounding tissue and, eventually, other organs, to the point where surgery alone can no longer do the job and more aggressive interventions — radiation among them — become necessary (Matthews et al., 2017). That progression is really the crux of why early detection matters so much here: cost and mortality both climb, sometimes steeply, as the disease advances from Stage I toward Stage IV. The flip side is encouraging, though. Caught early enough, something as comparatively simple as surgical removal of the lesion can be enough to keep the cancer from spreading further (Celebi et al., 2007). So the question isn't really whether early detection helps — it clearly does — it's how to get there reliably and at scale.
Right now, two methods dominate clinical practice: dermoscopy and biopsy. Dermoscopy-assisted diagnosis (Saurat, 2004) is useful, but it leans heavily on the skill of whoever is holding the instrument — and this is where things get a little uncomfortable. In less experienced hands, dermoscopy doesn't just fail to help; it can actually make diagnostic accuracy worse rather than better. Add to that the basic subjectivity of human interpretation — two dermatologists can, and sometimes do, read the same image differently — and it starts to become clear why interest in computer-assisted diagnosis has been building. Biopsy, the other standard option, brings its own baggage: it's invasive, slow, and by most patients' accounts, unpleasant.
This is roughly the gap computer-aided methods have tried to step into. Deep learning in particular has attracted attention, mostly because it can pull relevant features out of raw images on its own, without someone hand-engineering what to look for — and it has, by now, a fairly solid track record of doing this well. Several studies have shown that computer vision and machine learning techniques can diagnose pigmented skin lesions both accurately and, just as importantly, practically (Glaister, 2013; Celebi et al., 2007; Celebi et al., 2015; Hoffmann et al., 2003; Amelard et al., 2014). What's emerged is an end-to-end pipeline that trims both the cost and the time involved in screening. And there's a broader trend feeding into this too — smartphones. As their cameras have gotten sharper and more capable, AI-based screening applications have started to look genuinely viable, offering people a way to get an initial assessment without necessarily making a hospital visit first. For families who might otherwise face barriers — distance, cost, time — that kind of accessibility isn't a minor convenience; it can be the difference between catching something early and not catching it at all. All of which is to say: building reliable AI systems for skin lesion diagnosis isn't just an academic exercise. It has real, practical weight behind it.
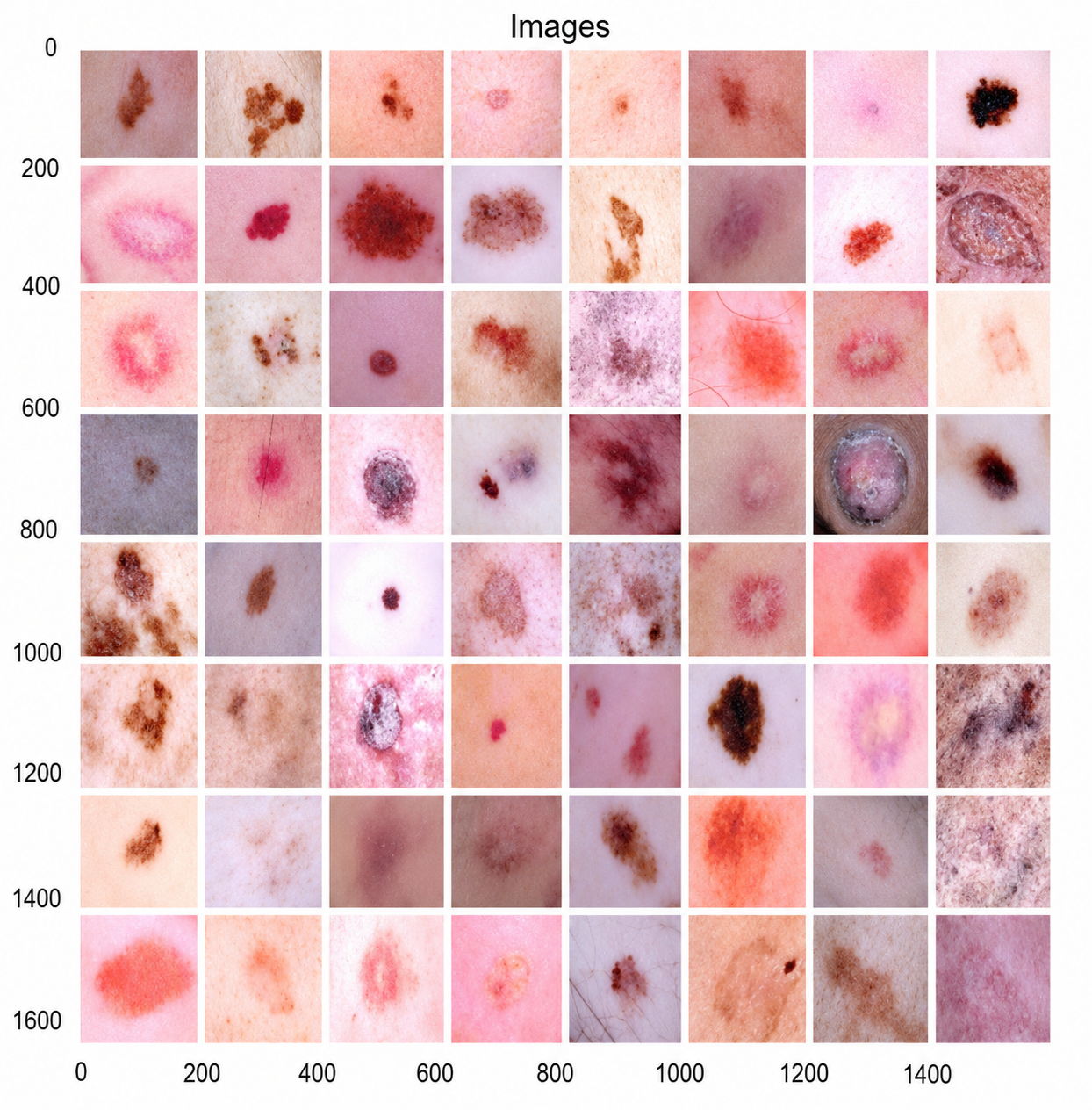
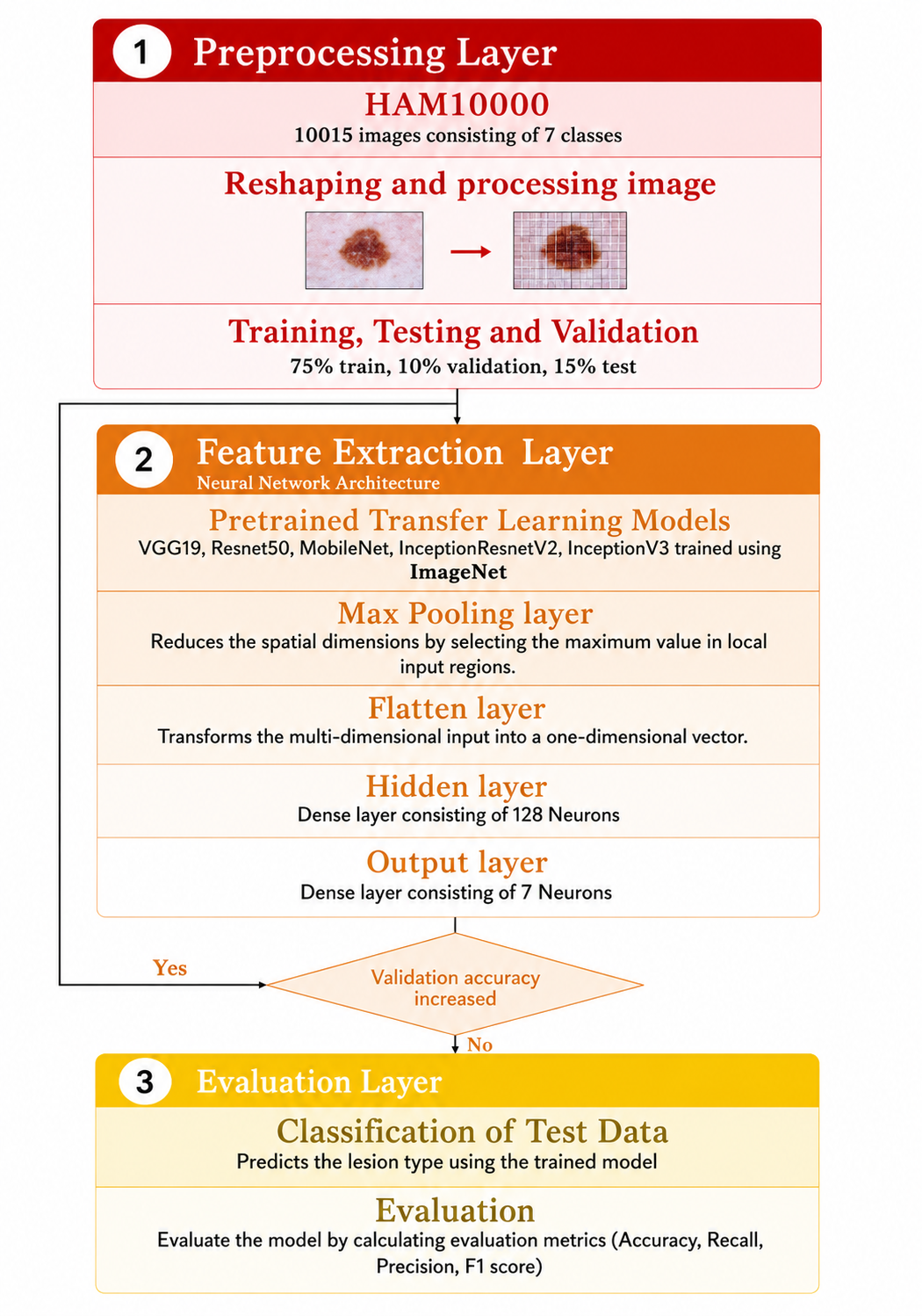
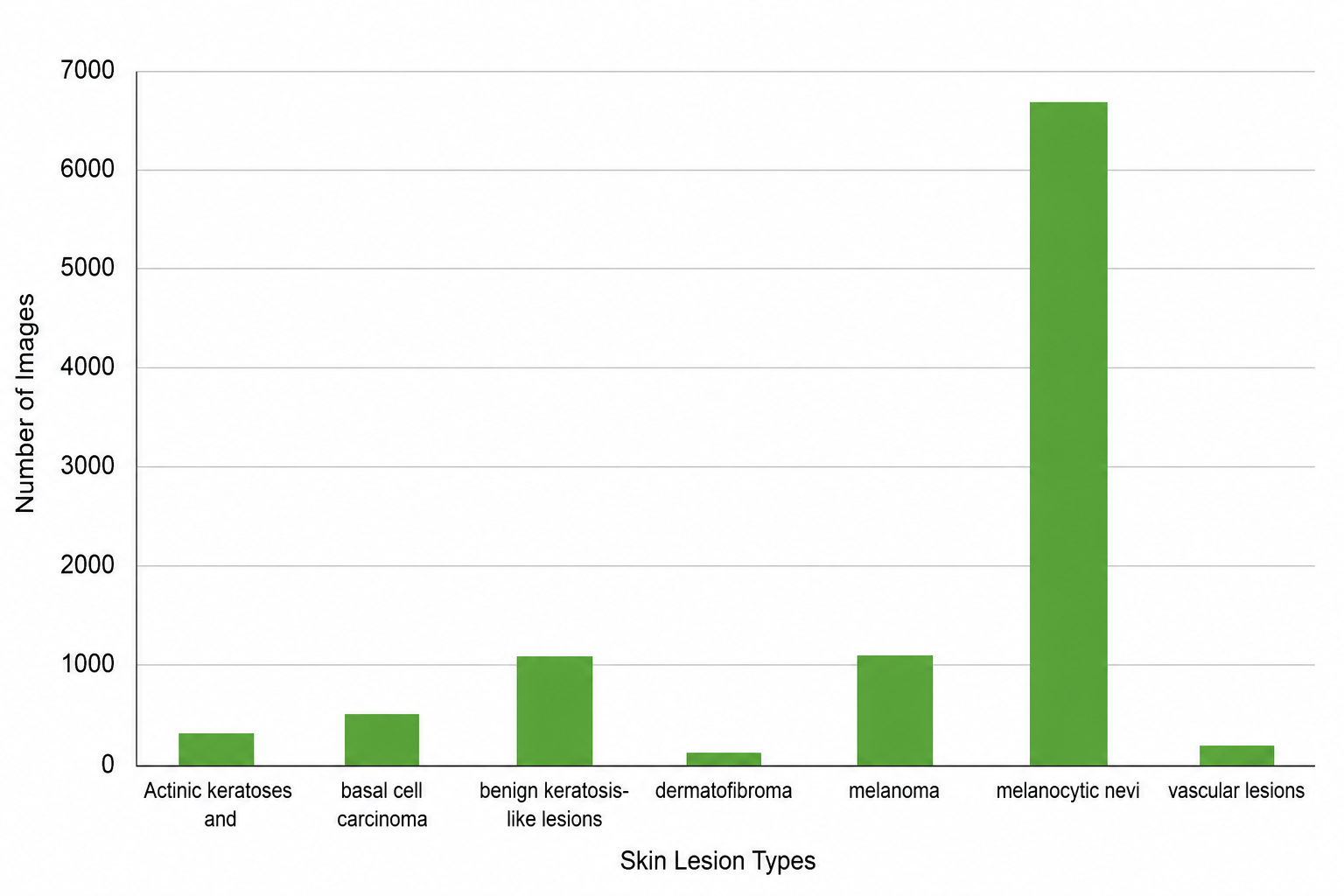
With that motivation in mind, this work sets out to compare five different transfer learning architectures on the task of multi-class skin cancer classification, using the HAM10000 dataset (Tschandl et al., 2018). The five models under consideration are VGG19, ResNet50, MobileNet, Inception-ResNetV2, and InceptionV3 — a fairly representative spread of architectures that have each, in their own way, shaped image classification research. Rather than simply reporting whichever model happens to score highest, the aim here is a genuine side-by-side comparison across accuracy and several other performance measures. As it turns out, MobileNet came out ahead — not by a small margin either, reaching 82.5% accuracy and outperforming every other model on precision, recall, and F1 score as well. That result is worth sitting with for a moment, since MobileNet is generally the "lighter," more efficient architecture of the group; that it still came out on top says something about the trade-off between model size and real-world performance that's worth exploring further.
The rest of the paper follows a fairly conventional structure, though each section earns its place. It opens with a look at existing machine learning and deep learning work on skin cancer detection, along with the datasets that have typically been used — partly to situate this study within that broader body of work, and partly to make clear what gaps remain. From there, the paper walks through the methodology behind the proposed comparative approach. Following that, the results are examined in more depth, with an eye toward not just the numbers themselves but what they suggest about each architecture's suitability for this kind of task. The paper closes by drawing together conclusions and pointing toward directions future research might reasonably take.
None of this happens in a vacuum, of course. The broader progress made in deep learning over the last decade (LeCun et al., 2015) has fed into a wide range of clinical decision-support systems, from diabetic retinopathy prediction to CT-based diagnostics (Kumar et al., 2015; Arcadu et al., 2019; Gunraj et al., 2020), and skin cancer detection has been very much part of that wave. Several recent reviews have taken stock of where things stand. Dildar et al. (2021) and Li et al. (2021), for instance, each conducted fairly comprehensive surveys of deep learning-based techniques for skin cancer detection, working through the range of methodologies in use, the datasets researchers have relied on, and — perhaps most usefully — the challenges that still haven't been fully resolved. Their work highlights the effectiveness of deep learning approaches for skin cancer detection, while also being honest about where the field still has work to do. It's within that same spirit — building on what's known, while being clear-eyed about what isn't yet settled — that this study positions itself.