1. Introduction
Segmenting the liver automatically, and doing it well, is not really optional anymore — it is the first link in almost every chain of AI-assisted liver diagnostics that follows. Without a dependable boundary around the organ, nothing downstream (tumor detection, volumetry, staging) has much to stand on. And yet the task resists easy solutions. Part of the difficulty is anatomical: the liver's shape, size, and position shift noticeably from one patient to the next, and even more so once disease enters the picture (Liu et al., 2019; Peng et al., 2014). Part of it is simply geographic — the organ sits crowded against the stomach, kidneys, and diaphragm, so an algorithm has to learn where the liver stops and its neighbors begin, often across blurry, low-contrast margins.
Clinically, when the question is liver pathology, most radiologists reach for magnetic resonance imaging rather than CT, largely because MR offers a level of soft-tissue contrast and spatial detail that CT struggles to match (Alves et al., 2007; Wang et al., 2019). That preference, though, creates an odd asymmetry in the segmentation literature. CT-based deep learning pipelines have had a fairly easy path to strong performance, in large part because Hounsfield units give every CT scan a shared, standardized intensity scale — and once you have that, contrast enhancement and normalization become almost mechanical (Kim & Chun, 2020). MRI offers no such gift. Intensity values on an MR scan are scanner-dependent, sequence-dependent, even patient-dependent, and there is no universal "Hounsfield-like" reference to lean on. So the same segmentation accuracy that CT models reach fairly routinely has, historically, been much harder to reproduce on MR data.
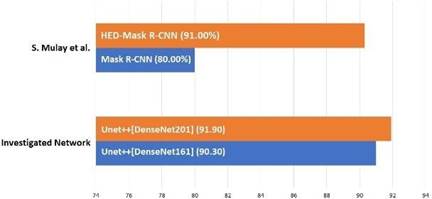
This gap has not gone unnoticed. Xiang et al. (2021), reviewing the broader field of deep-learning-driven liver imaging, pointed out that liver segmentation performance from MRI still lags meaningfully behind CT-based results, and — perhaps more tellingly — that comparatively little rigorous work had been done in the MRI space at all (Xiang et al., 2021). A handful of studies have tried to close that distance in different ways. Mostafa et al. (2017), for instance, took a rather different route from the deep-learning mainstream and applied a whale optimization algorithm to the liver-segmentation problem on MR scans (Mostafa et al., 2017). Mulay et al. (2019) instead combined geometric edge-enhancement with a Mask R-CNN framework, an approach that leaned on boundary information more explicitly than most CNN pipelines do (Mulay et al., 2019). More recently — and arguably setting the benchmark this study measures itself against — Zbinden et al. (2022) applied nnUNet to T1-weighted MRI slices and reported the strongest results yet on this class of problem (Zbinden et al., 2022).
It is worth pausing on why CT-focused work has moved faster, because the contrast is instructive rather than just historical trivia. Tang et al. (2020) reported a dice similarity coefficient near 98% for whole-liver segmentation from plain CT using a modified multiscale CNN (Tang et al., 2020), and Hu et al. (2016), working with a three-dimensional CNN, landed a DSC around 97.25% on a comparable task (Hu et al., 2016). Both groups leaned on Hounsfield-unit scaling during preprocessing — precisely the tool that MRI does not offer. So the numbers are not just a story about better architectures; they are, at least in part, a story about better-behaved input data. That distinction matters here, because it reframes the problem: closing the MRI-CT gap may depend as much on preprocessing and enhancement strategy as on network design itself.
That reframing is really the starting point for this study. If MRI cannot borrow CT's built-in intensity standardization, perhaps something functionally similar can be engineered on the MR side — through contrast manipulation, through channel construction, through whatever preprocessing tricks make the liver's boundary easier for a network to "see." T1-weighted sequences offer a useful foothold here: fat and protein content appear brighter under T1 weighting, which tends to make the liver stand out more clearly against its surroundings than it would under other sequence types. That single property is, in a sense, a natural advantage worth exploiting rather than a curiosity worth noting in passing.
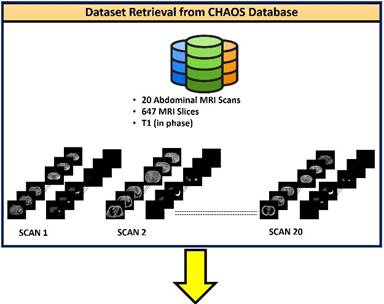
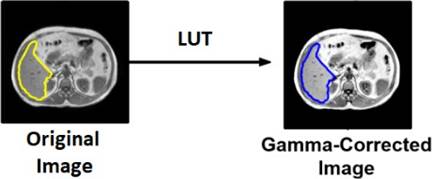
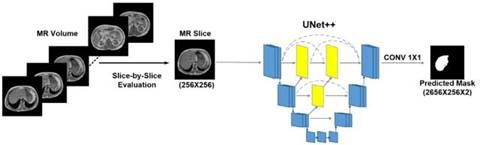
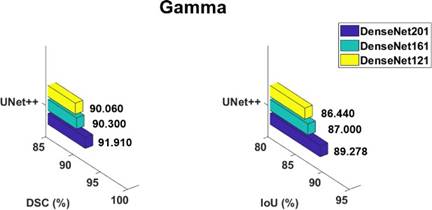
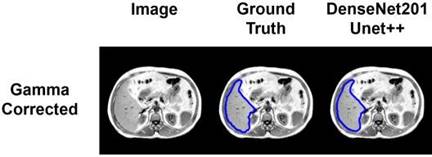
With that in mind, this work investigates the UNet++ architecture, paired with DenseNet encoder-decoder backbones of varying depth, for liver segmentation from volumetric T1-weighted abdominal MRI. The choice is not arbitrary — UNet++'s nested skip pathways were designed precisely to recover the kind of fine boundary detail that plain U-Net architectures tend to blur, which is exactly the failure mode liver segmentation is prone to given its ambiguous organ margins. Alongside the architecture question, this study also asks a preprocessing question: does image enhancement — contrast stretching, adaptive stretching, gamma correction, and RGB channel construction — meaningfully change segmentation performance on T1-weighted slices, and if so, which enhancement pairs best with which network configuration?
Taken together, the aim is fairly direct, even if the path to it required a few different threads to pull. This study sets out to (1) systematically evaluate state-of-the-art segmentation architectures on T1-weighted abdominal MR liver segmentation, (2) quantify how different image-enhancement pipelines affect that performance, and (3) benchmark the resulting approach against prior work on the same public dataset. The hope, ultimately, is not just an incremental accuracy gain, but a segmentation pipeline reliable enough to genuinely support — rather than merely gesture toward — AI-assisted liver pathology diagnosis from MRI.