1. Introduction
Parkinson's disease rarely announces itself all at once. It tends to arrive in small, easily dismissed ways — a hand that trembles slightly while resting, handwriting that gets a little smaller, a step that doesn't quite swing the way it used to. By the time these signs are obvious enough to bring someone into a clinic, the underlying neurodegeneration has often been progressing for years. This is, in some sense, the central frustration of Parkinson's disease (PD) care: the disease is defined clinically by motor symptoms, yet those symptoms are late arrivals, not early warnings.
PD is a progressive neurological disorder marked by tremor, rigidity, bradykinesia, and postural instability (Singh, Pillay, & Choonara, 2007), and its symptoms typically worsen gradually rather than appearing in full force. Diagnosis, as it stands, leans almost entirely on these motor signs — which is part of the problem. Motor symptoms generally don't surface until a substantial portion of dopaminergic neurons in the substantia nigra has already been lost (Sharma et al., 2013). So, in practice, many people live with PD for some time before anyone — including the person experiencing it — recognizes what's happening.
Why does earlier detection matter so much? A few reasons, and they compound. First, there's the treatment angle: neuroprotective interventions, where they exist or are being trialed, tend to work best before extensive neuronal loss has occurred (Singh et al., 2007) — so timing matters enormously. Second, an earlier diagnosis gives patients room to make lifestyle adjustments (diet, exercise, and so on) that may help slow symptom progression, even modestly. And third, earlier detection gives clinicians a longer runway to track how the disease is unfolding in a given patient and adjust treatment accordingly, rather than reacting to a disease that's already well established. Efforts using predictive modelling combined with patient questionnaires, as well as broader multimodal feature sets, have already demonstrated the feasibility of identifying PD at an early, pre-clinical stage (Prashanth & Roy, 2018; Prashanth, Roy, Mandal, & Ghosh, 2016).
None of this is news to the research community, of course. Over the past decade or so, a fairly broad effort has emerged around finding more reliable early markers for PD — some of it biological, some of it computational. On the biological side, attention has gone toward biomarkers such as genetic variants, alpha-synuclein levels, neuroimaging signatures from dopamine transporter studies, and cerebrospinal fluid composition (Sharma et al., 2013). Imaging techniques like PET and SPECT have also proven useful for visualizing the kinds of degenerative changes associated with PD, sometimes before motor symptoms become pronounced. And clinically, tools like the Unified Parkinson's Disease Rating Scale (UPDRS) remain the standard for tracking motor symptom severity, even as researchers increasingly look toward non-motor signs — sleep disturbances, loss of smell (Silveira-Moriyama et al., 2009), subtle cognitive shifts, and autonomic changes such as altered cardiovascular oscillations (Valenza et al., 2016) — as potentially earlier indicators.
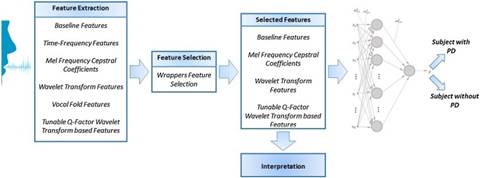
What's changed more recently, though, is the role of machine learning. Rather than waiting for a single definitive biomarker, researchers have started asking whether combinations of data — clinical records, imaging, sensor data, even voice recordings — might collectively reveal patterns that no single measure would show on its own. Voice and speech analysis has been a particularly active area: dysphonia measures have been shown to be suitable for telemonitoring PD progression (Little, McSharry, Hunter, Spielman, & Ramig, 2009; Tsanas, Little, McSharry, & Ramig, 2010), and numerous classification approaches have been built on top of these signals, including support vector machines applied to ranked voice features (Lahmiri & Shmuel, 2019), deep learning models trained on vocal feature sets (Gunduz, 2019), acoustic analyses of speech (Braga, Madureira, Coelho, & Abraham, 2019), and small, curated sets of vocal features used as a pre-diagnosis screening tool (Solana-Lavalle, Galán-Hernández, & Rosas-Romero, 2020). Practical concerns around real-world deployment — such as the reliability of pitch-detection algorithms across noise conditions when speech is captured on a smartphone — have also been examined (Illner, Sovka, & Rusz, 2020).
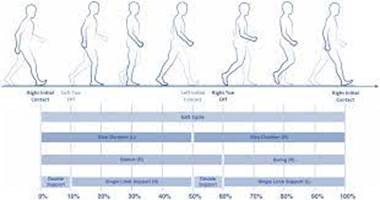
Gait has formed a second major strand of this work: hybrid spatio-temporal models have been used to both detect PD and rate its severity from gait data (Zhao, Qi, Li, Dong, & Yu, 2018), and deep one-dimensional convolutional networks have been applied to the same task with strong results (El Maachi, Bilodeau, & Bouachir, 2020). Handwriting represents a third, with decision-support frameworks built around novel handwriting markers (Drotár et al., 2015), kinematic and pressure-based analyses used for differential diagnosis (Drotár et al., 2016), and sex-specific, age-adjusted classification models derived from handwriting measurements (Gupta, Bansal, & Joshi, 2020).
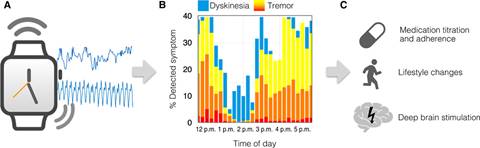
Mobile health technologies have played a notable part in this shift. Mobile applications have already been explored for PD diagnosis and ongoing monitoring (Mamun et al., 2017), touchscreen typing dynamics have been used to detect motor impairment via everyday smartphone use (Arroyo-Gallego et al., 2017), wavelet-based methods have been proposed for monitoring symptoms through wearable sensors (Wagner, Fixler, & Resheff, 2017), and long short-term memory networks have been applied to patient-specific detection of freezing of gait (Ashour, El-Attar, Dey, El-Kader, & Abd El-Naby, 2020). More broadly, large-scale predictive analytics frameworks have shown how heterogeneous, multi-source PD data can be combined (Dinov et al., 2016), comparative studies have benchmarked multiple classification algorithms for PD diagnosis (Das, 2010), and methodological advances in feature extraction for related neurodegenerative conditions such as ALS (Bilgin, 2017), as well as in statistical, data-driven monitoring more generally (Harrou, Sun, Hering, & Madakyaru, 2020), have helped shape how such models are designed and validated. And more broadly, sensor-based approaches have gathered momentum as a way of capturing real-world, longitudinal data about how the disease behaves outside the clinic. The practical obstacle, though, is that many of these systems require multiple dedicated devices, which limits how realistically they can be used day-to-day. Consumer smartwatches — with their built-in triaxial accelerometers — offer a more accessible alternative, and multitask classification models have been proposed specifically to assess the magnitude and consistency of resting tremor using this kind of off-the-shelf hardware (Sigcha et al., 2021).
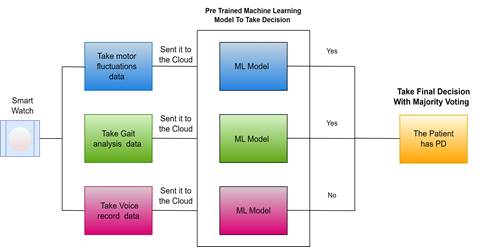
It's this last thread — accessible, wearable, continuously-collected data — that motivates the present work. Rather than relying on a single signal type, we set out to build a model that draws on three complementary streams from a single smartwatch: motor fluctuations, gait characteristics, and voice recordings. Each of these has, individually, shown some promise for PD-related signal detection in prior work; what's less explored is how they might work together. The data from all three sensors is sent to the cloud, where a pretrained machine learning model evaluates it, and an ensemble approach combines the outputs of the three modalities through majority voting to arrive at a final decision. The sections that follow describe the reasoning behind each component, the methods used, and what the preliminary results suggest — along with, candidly, what they don't yet show.