2.1 Design
This is a narrative review, not a systematic review or meta-analysis, and we state that plainly here rather than let readers infer it from the absence of a PRISMA flow diagram. We chose this design because the underlying literature on telesurgical feasibility is overwhelmingly descriptive, simulation-based, or framework-proposing rather than comparative-trial based; forcing a quantitative synthesis onto that evidence base would have implied a precision the literature does not actually support. That said, we have tried, wherever practical, to document our process with enough specificity that another team could substantially retrace it — a standard closer to what would be expected of a scoping review, even if we stop short of claiming that label formally.
2.2 Information Sources and Search Strategy
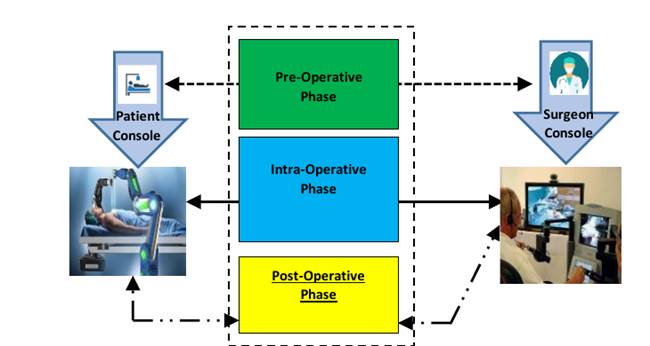
Figure 1: Schematic overview of a telesurgical system architecture, illustrating the surgeon console and patient console and their constituent functions (display, haptic feedback, camera and communication control on the surgeon side; vital-sign monitoring, surgical-site imaging, and emergency-stop functionality on the patient side) across the pre-operative, intra-operative, and post-operative phases of a remote surgical procedure.
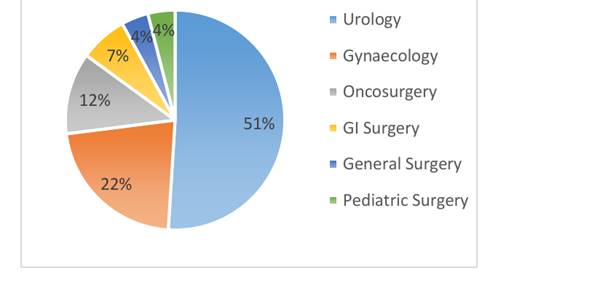
Figure 2: Distribution of robotic surgery cases across medical specialties, showing the proportional share attributable to urology, gynaecology, oncosurgery, and other specialties. Data adapted from Sinha et al. (2021).
Table 1: Comparative overview of major telesurgical and surgical robotic platforms developed worldwide, 1991–2022, detailing year of introduction, manufacturer, country of last documented use, technical description, advantages, and disadvantages. Adapted from Gupta et al. (2019) and cross-checked against manufacturer and regulatory documentation.
|
Name of the Robot
|
Year
|
Company
|
Country (Last Used)
|
Description
|
Advantages
|
Disadvantages
|
|
Medrobotics
|
1991
|
Flex Robotic Systems
|
USA (1991)
|
Used for stereotactic brain surgery with improved accuracy
|
Surgeons’ choice of implants
|
Not suitable for colorectal applications
|
|
ROBODOC
|
1992
|
Integrated Surgical Systems, Inc., Sacramento, CA
|
Canada (1995)
|
Used for hip replacement
|
Safe surgery
|
High cost
|
|
MKM system
|
1993
|
Zeiss, Germany
|
Germany (2001)
|
During neurosurgical procedures, this robotic microscope was utilized.
|
A complete robotic solution for stem and cup
|
No external safety
|
|
ZEUS robotic Surgical System
|
1994
|
Computer Motion Ltd., USA
|
USA (2001)
|
Tubal re-anastomosis
|
Get rid of templates that are less accurate and adopt jig-based technology.
|
Accuracy
|
|
RAMS Robot
|
1995
|
NASA, USA
|
USA (2001)
|
Compatible with MRI
|
Open-platform surgical system
|
No real-time services for information updates
|
|
The Steady Hand system
|
1995
|
John Hopkins University, Maryland
|
USA (2000)
|
Detects pressure put by the surgeon in neurosurgery
|
Precise pre-surgical planning is executed every time
|
No sufficient range of motion is required for general-purpose surgery
|
|
ZEUS Robot
|
1998
|
Computer Motion Ltd., USA
|
USA (2001)
|
Surgery without cardiac bypass
|
Precise computer-assisted preparation of the bone cavity and joint surfaces
|
No Tactile feedback
|
|
Da Vinci Robotic Surgery System
|
1998
|
Intuitive Surgical
|
USA (2000)
|
Used to harvest the internal thoracic artery
|
Rich in technically. Available experienced surgeons at all locations
|
Most physicians performing prostate surgery have not been trained in this procedure.
|
|
Da Vinci Surgical System
|
2000
|
Intuitive Surgical
|
USA (2014)
|
Performing surgeries with a minimally invasive approach, even for complex cases.
|
Patients who undergo this medical procedure experience lower risk of complications, reduced blood loss, fewer transfusions, and less pain.
|
Adverse effects, such as incontinence and erectile dysfunction, may occur and there is a risk of blood clots and infection.
|
|
Da Vinci Robot
|
2000
|
Intuitive Surgical
|
USA (2014)
|
Complicated gynecological surgeries
|
Non-optical technology
|
Only used for gynecological surgeries
|
|
Vascular Robotic System
|
2002
|
Corindus Corpath
|
USA (2014)
|
Perform percutaneous coronary interventions
|
Achieves full potential with forward-thinking physicians
|
Not progressed as rapidly as endovascular technology
|
|
Pathfinder Robot
|
2004
|
Armstrong Healthcare Ltd
|
UK (2016)
|
Proper guidance for the surgeons
|
Sub-millimeter dimensional accuracy
|
Used old technology
|
|
Senhance surgical robotics system
|
2006
|
Asensus Surgical, Inc.
|
USA (2023)
|
Laparoscopic Surgery
|
Advanced eye sensing camera, Haptic feedback, Direct visual contact, and reasonable cost
|
Limited procedural time for surgical field
|
|
The NeuroArmSYMBIS Robot
|
2007
|
IMRIS, USA
|
USA (2023)
|
MRI-based robot to remove brain tumor
|
Precise milling services to ensure optimal alignment.
|
Used only for brain tumor
|
|
ROSA
|
2007
|
Medtech, France
|
France (2022)
|
Brain surgery procedures
|
High-precision smart-tool technology, freedom of movement, and advanced assisted navigation.
|
Tearing or puncturing of vessels or internal organs
|
|
Renaissance Guidance System
|
2007
|
Mazor Robotics
|
Israel (2023)
|
Offers a direct blueprint for the surgical process and is tailored to each patient
|
Better precision during surgeries, ultimately leads to a decrease in complication rates and quicker recovery periods for patients.
|
Only used for spine surgery
|
|
Smart Tissue Autonomous Robot (STAR)
|
2009
|
Johns Hopkins University
|
USA (2020)
|
A corrected 3D model with multiple camera views was created using plenoptic imaging.
|
Stitching, sewing, looping, and threading
|
The camera was not fast enough to track tissue deformation accurately in real-time.
|
|
Mako Rio robot
|
2009
|
Stryker
|
USA (2023)
|
Used for partial knee replacements and hip surgeries
|
Immediate pain relief, less blood loss, and shorter hospital stays following hip or knee surgery.
|
May cause hip-joint misalignment
|
|
TSolution One
|
2014
|
Think Surgical, Inc.
|
USA (2017)
|
For orthopedic surgical procedures for the hip
|
Personalized pre-surgical plans
|
No differentiation between tissue types
|
|
DaVinci Xi robotic surgery
|
2014
|
Intuitive Surgical
|
USA (2023)
|
Involves minimal invasion during the procedure.
|
Perform multiple surgeries
|
Vision and motor functions were not included
|
|
Miniature Robot
|
2016
|
Virtual Incision Corp
|
USA (2023)
|
This is used to treat patients with Crohn’s disease, colon cancer, diverticulitis, and ulcerative colitis.
|
Achieving a quicker and more efficient recovery.
|
Climate uncertainty
|
|
Epoch robotic surgery system
|
2018
|
Stereotaxis
|
USA (2020)
|
Magnets are used to control catheters that are inserted into the heart for manipulation.
|
Minimize x-ray exposure by up to 90% during procedures and enhance the capacity to treat intricate rhythms.
|
Not suitable for preoperative data
|
|
Navio surgical system
|
2018
|
Smith & Nephews
|
UK (2023)
|
Partial knee replacement
|
Faster recovery time, less pain, smaller incisions, and natural knee motion during rehabilitation.
|
Uni-compartmental Knee Replacement
|
|
SSI Mantra
|
2022
|
SS Innovation Pvt. Ltd.
|
India (2023)
|
For general surgery, used in a cancer institute
|
The design of the console is open-faced, modular, flexible, versatile, and has UPS backup.
|
Limited development time
|
We searched four databases — Google Scholar, IEEE Xplore, PubMed, and ScienceDirect — between [search dates to be specified by authors], supplemented by manual screening of the reference lists of key articles (snowball sampling). Search terms combined free-text keywords joined with Boolean operators, including combinations of "robotic surgery," "telesurgery," "opportunity," "challenges," and "Bangladesh" (e.g., ("telesurgery" OR "robotic surgery") AND ("challenges" OR "opportunity" OR "feasibility") AND ("Bangladesh" OR "low- and middle-income countries")). We did not restrict by document type at the outset; conference proceedings, peer-reviewed journal articles, and preprints (notably arXiv) were all eligible for screening, since a meaningful share of the more technically rigorous cybersecurity work in this space circulates first as a preprint (Takanashi et al., 2023).
2.3 Eligibility Criteria
The publication window was bounded to 2018–2023, with one deliberate exception: Bonaci et al. (2015), which we retained outside the window because it appears to be among the earliest empirical demonstrations of an adversarial attack — specifically, a distributed denial-of-service attack — against a telesurgical platform in a controlled setting. Excluding a foundational study on recency grounds alone struck us as a decision that would weaken, rather than strengthen, the review.
Studies were eligible if they addressed telesurgical feasibility, technical architecture (including 4G/5G and tactile-internet implementations), cybersecurity vulnerabilities or countermeasures, or clinical specialty-level adoption patterns. We excluded studies focused primarily on blockchain-based security mechanisms, on the judgment — a qualitative one, not a statistical one, and we say so plainly — that such approaches introduce a level of computational and procedural complexity disproportionate to their real-world deployability in low-resource settings.
2.4 Study Selection
Title and abstract screening was performed independently by both authors, with a preference for open-access articles or those to which institutional access permitted full-text retrieval. This is a pragmatic constraint rather than a methodological ideal, and we disclose it rather than gloss over it, since access barriers of this kind shape what gets cited in resource-limited settings just as concretely as they shape what gets practiced clinically. From an initial pool in the low thousands of titles — we did not track an exact figure, which we acknowledge here as a limitation rather than defend as adequate — twelve articles were retained for full-text synthesis based on relevance to telesurgical feasibility, technical architecture, or cybersecurity (Table 2).
2.5 Data Extraction
For each of the twelve included sources, we extracted, where reported: study focus, telesurgical platform or protocol under discussion, network technology (4G/5G/tactile internet), reported latency figures, identified security vulnerabilities, and proposed mitigations. Extraction was performed independently by both authors and reconciled by discussion; disagreements were resolved by consensus rather than a third-reviewer arbitration process, which we note as a further methodological limitation appropriate to a two-author team.
To characterize the historical landscape of surgical robotics platforms more broadly, we additionally compiled a comparative table (Table 1) adapted from the architecture survey by Gupta et al. (2019), cross-checked against manufacturer and regulatory documentation where publicly available.
2.6 Cost and Contextual Data
Cost estimates for telesurgical infrastructure — acquisition costs and the recurring cost of high-bandwidth network access — were drawn from publicly available technical and encyclopedic sources (Wikipedia, n.d.), given the absence of standardized, peer-reviewed pricing data in this space. We flag this explicitly as a methodological soft spot: these figures should be read as directional estimates rather than validated data points, and we would encourage future work to seek out procurement records or manufacturer disclosures as a more authoritative alternative.
2.7 Synthesis Approach
Findings were organized thematically rather than chronologically, around three axes that emerged inductively from the included literature: (a) opportunities for telesurgical deployment in low- and middle-income country settings, (b) technical, regulatory, and ethical barriers, and (c) candidate interventions, contextualized specifically for Bangladesh's infrastructural and policy
Table 2: Summary of the twelve studies included in this narrative synthesis, listing publication year and primary focus area (e.g., telesurgical feasibility, network architecture, cybersecurity vulnerabilities and countermeasures, clinical implementation), alongside the focus area of the present study for comparison.
|
Paper
|
Title
|
Year
|
Focus Area
|
|
[1]
|
Foreseeable challenges in developing telesurgery for low-income and middle-income countries
|
2021
|
Telesurgery, Challenges, LMIC, Opportunities
|
|
[2]
|
Tactile-internet-based telesurgery system for healthcare 4.0: An architecture, research challenges, and future directions
|
2019
|
Telesurgery, 5G, tactile internet, latency, reliability
|
|
[3]
|
The feasibility of utilizing Telesurgery Service in the Autonomous Region of the Azores, with the support of 5G network.
|
2023
|
Telesurgery, 5G, remote surgery, feasibility, benefits
|
|
[4]
|
Protecting procedural care—cybersecurity considerations for robotic surgery
|
2022
|
Robotic surgery, cybersecurity, vulnerabilities, security measures
|
|
[5]
|
Telesurgery and robotics: an improved and efficient era
|
2021
|
Telesurgery, 5G networks, haptic feedback, tactile robotics, Internet of Things (IoT)
|
|
[6]
|
Cyber-Secure Teleoperation With Encrypted Four-Channel Bilateral Control
|
2023
|
Telesurgery, Challenges, Cybersecurity, Encryption
|
|
[7]
|
Experimental analysis of denial-of-service attacks on teleoperated robotic systems
|
2015
|
Telesurgery, DOS, Cybersecurity, Experimental Analysis
|
|
[8]
|
On cyber-physical attacks in bilateral teleoperation systems: An experimental analysis
|
2018
|
Telesurgery, Challenges, Cybersecurity, Experimental Analysis
|
|
[9]
|
RT-TelSurg: Real-time telesurgery using SDN, fog, and cloud as infrastructures
|
2021
|
Robotic surgery, cybersecurity, vulnerabilities, security measures, SDN, FOG, Cloud
|
|
[10]
|
SecureSurgiNET: A framework for ensuring security in telesurgery
|
2019
|
Telesurgery, Challenges, Cybersecurity, tactile robotics, Security Framework
|
|
[11]
|
Telesurgery robot based on 5G tactile internet. Mobile Networks and Applications
|
2018
|
Telesurgery, 5G networks, haptic feedback, tactile robotics, Internet of Things (IoT)
|
|
[13]
|
Robotic surgery in paediatric patients: Our initial experience and roadmap for successful implementation of robotic surgery programme
|
2021
|
Robotic Surgery, Medical Specialties, Implementation challenges.
|
|
Our Paper
|
Feasibility of Robotic Surgery: Opportunities and Challenges in Bangladesh
|
2023
|
Robotic Surgery, Bangladesh, Challenges, Opportunities, Recommendations
|
environment. No formal quality-appraisal instrument (e.g., GRADE, Newcastle-Ottawa) was applied, consistent with the narrative nature of this review; we consider this an area future iterations of this work should address directly, particularly if the intent is eventual publication in a venue that expects formal risk-of-bias assessment.
